NHS eReferral service
Reducing clinical risk by making system experience improvements
Situation
Clinical systems are renowned for having poor usability and performance issues, but NHS Digital are leading the way in what good should look like. As a user centred designer at NHS Digital, I was responsible for the end-to-end system experience of the e-Referral service, used by clinicians and admin staff.
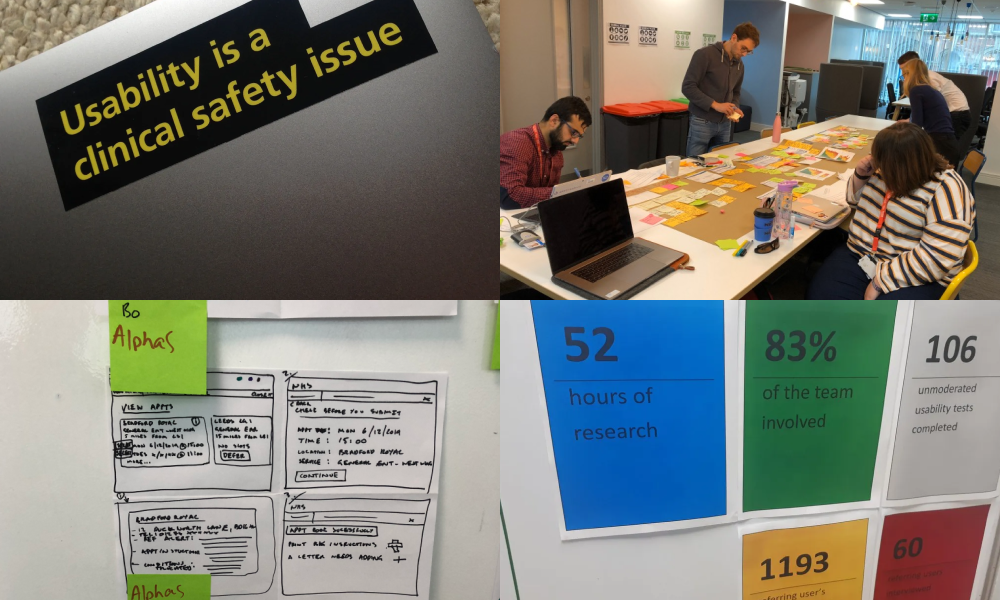
The e-Referral service allows clinicians to offer patients a choice when booking appointments, giving them freedom, convenience and confidence at the point when care is needed, or even critical. We juggled policy intent with user needs in an area of the NHS where clinical input is critical to minimise risk to patient care, and where usability is itself a clinical safety issue.
Process
My product team put user needs first, as they are key to getting services and systems right. In the short time on the e-Referral programme, we changed how the team worked by focussing on the tried and tested double diamond process, with discovery and alpha phases at the heart of our agile cadence.
As a product team, we diverged on separate but directly related areas of work as part of a single user flow, working through story mapping, design sprints, problem statement and hypothesis generation, prototyping with the NHS kit, usability testing, and iterating on metrics including SUS and SEQ scores.
Focussing on the problem
I challenged the team to move away from implementing suggested solutions and ideas, and instead to focus on the problem statement at hand. We did this by mapping out the existing steps of a flow, creating a story map of the digital service from the user's perspective, and highlighting known pain points to focus on as part of the redesign.
We used metrics and data to evidence decision making, analysing user feedback and analytics to feed into the confidence we had in each design iteration. This also helped during show and tells, giving the wider team insight into how things were shaping up.
Result
The scope and impact of what we did was significant. We worked with our own NHS Standards team, NHSBSA, Summary Care Records, different hospital trusts, as well as GOV designers — collaborating, sharing, asking questions, and learning from each other.
Our team was among the first to contribute back to the NHS service manual upon its inception, ensuring other teams could find what we did useful for their own service, and solve similar problems in a consistent way.
We delivered a simpler clinical system for booking patient appointments, more confident staff, and more time for doctors to focus on patients.